


5 minutes read, PDF version available: DOWNLOAD PDF
How UV-C + Indoor Air Quality Upgrades Help Senior Living Communities Protect Residents and Stabilize Operations.
When a resident becomes ill in a senior living community or nursing home, one question quickly arises for the care team: how many more people might become sick in the next few days?
That uncertainty is stressful for residents and families. It is disruptive for staff. And it can quickly raise the cost and complexity of care, from added clinical monitoring and infection-control measures to staffing strain, overtime, and increased cleaning and supplies.
For operators, the impact extends well beyond a single case. When respiratory illness spreads through a community, daily operations can shift rapidly from routine care to crisis management.
That’s why infection prevention and indoor air quality (IAQ) improvements are increasingly viewed as a core operational strategy: helping reduce avoidable illness so more residents can remain safely in their community and more care can be delivered in-house with fewer disruptions.
IAQ AS AN OPERATING STRATEGY
Since the 1940s, schools and hospitals have used germicidal ultraviolet energy (GUV or UV-C) to reduce the airborne transmission of infectious diseases by inactivating bacteria and viruses as they circulate through indoor air.
Historic field studies in U.S. schools showed that upper-room UV systems significantly reduced measles transmission among children by disinfecting the air where respiratory particles accumulated. These early public-health successes demonstrated that airborne infection control could protect entire classrooms without requiring direct behavioral interventions.
Today, similar principles are being applied in healthcare and congregate living environments.
Ownership teams don’t need to understand the physics of UV wavelengths to appreciate the operational value of cleaner air. What matters is the outcome: healthier residents, steadier staffing, and fewer disruptions across the community.
Airborne illness creates ripple effects throughout assisted living environments. When respiratory viruses spread, the impact is felt far beyond the initial case.
Staff absences increase. Care teams spend more time on monitoring and isolation protocols. Supplies such as oxygen, PPE, and testing materials are consumed more quickly.How UV-C + Indoor Air Quality Upgrades Help Senior Living Communities Protect Residents and Stabilize Operations.
When a resident becomes ill in a senior living community or nursing home, one question quickly arises for the care team: how many more people might become sick in the next few days?
That uncertainty is stressful for residents and families. It is disruptive for staff. And it can quickly raise the cost and complexity of care, from added clinical monitoring and infection-control measures to staffing strain, overtime, and increased cleaning and supplies.
For operators, the impact extends well beyond a single case. When respiratory illness spreads through a community, daily operations can shift rapidly from routine care to crisis management.
That’s why infection prevention and indoor air quality (IAQ) improvements are increasingly viewed as a core operational strategy: helping reduce avoidable illness so more residents can remain safely in their community and more care can be delivered in-house with fewer disruptions.
IAQ AS AN OPERATING STRATEGY
Since the 1940s, schools and hospitals have used germicidal ultraviolet energy (GUV or UV-C) to reduce the airborne transmission of infectious diseases by inactivating bacteria and viruses as they circulate through indoor air.
Historic field studies in U.S. schools showed that upper-room UV systems significantly reduced measles transmission among children by disinfecting the air where respiratory particles accumulated. These early public-health successes demonstrated that airborne infection control could protect entire classrooms without requiring direct behavioral interventions.
Today, similar principles are being applied in healthcare and congregate living environments.
Ownership teams don’t need to understand the physics of UV wavelengths to appreciate the operational value of cleaner air. What matters is the outcome: healthier residents, steadier staffing, and fewer disruptions across the community.
Airborne illness creates ripple effects throughout assisted living environments. When respiratory viruses spread, the impact is felt far beyond the initial case.
Clinical teams face added pressure, and routine services, from dining to activities, can be interrupted.
Hospital transfers add another layer of strain. Each transfer requires coordination with medical providers, documentation, family communication, and follow-up care planning when the resident returns.
Residents who leave the community for acute care may come back weaker and require additional support. Families experience stress and uncertainty, and staff must invest time helping residents regain stability.
In short, illness doesn’t just affect individual residents—it disrupts operations across the entire building.
Airborne infection-prevention strategies, including germicidal UV (GUV) air disinfection, aim to address this challenge at the source: the shared air residents and staff breathe throughout the day.
By reducing the concentration of airborne pathogens in common areas and HVAC systems, these technologies help limit the conditions that allow respiratory illnesses to spread.
Importantly for operators, these systems can often be deployed at relatively modest and predictable cost. For installations similar to the Cardigan Ridge pilot, the two-year total cost of ownership, including equipment, installation, and maintenance, averages approximately $1.89 per day per unit.
Compared with the operational disruption caused by outbreaks of respiratory illness, this type of investment is increasingly viewed as a practical component of infection-prevention infrastructure rather than a discretionary building upgrade.
Even modest reductions in illness can produce meaningful operational benefits.
Fewer infections mean:
Residents who leave the community for acute care may come back weaker and require additional support. Families experience stress and uncertainty, and staff must invest time helping residents regain stability.
In short, illness doesn’t just affect individual residents—it disrupts operations across the entire building.
Airborne infection-prevention strategies, including germicidal UV (GUV) air disinfection, aim to address this challenge at the source: the shared air residents and staff breathe throughout the day.
By reducing the concentration of airborne pathogens in common areas and HVAC systems, these technologies help limit the conditions that allow respiratory illnesses to spread.
Importantly for operators, these systems can often be deployed at relatively modest and predictable cost. For installations similar to the Cardigan Ridge pilot, the two-year total cost of ownership, including equipment, installation, and maintenance, averages approximately $1.89 per day per unit.
Compared with the operational disruption caused by outbreaks of respiratory illness, this type of investment is increasingly viewed as a practical component of infection-prevention infrastructure rather than a discretionary building upgrade.
Even modest reductions in illness can produce meaningful operational benefits.
Fewer infections mean:
- fewer staff call-outs
- fewer emergency clinical interventions
- fewer hospital visits
- more consistent daily routines for residents
Activities continue. Dining rooms remain open. Families feel more confident about their loved ones’ safety.
That is why many senior living operators are beginning to view indoor air quality as part of their infection-prevention infrastructure, alongside cleaning protocols, vaccination programs, and clinical monitoring.
The value of prevention often appears in what doesn’t happen: fewer disruptions, fewer escalations of care, and more days where residents can live comfortably and safely within their own community.

FIELD-TESTED AND UNIVERSITY-VERIFIED
To evaluate whether better indoor air can help prevent illness and reduce care disruptions, Light Progress launched a pilot project at Cardigan Ridge, a senior living community in Minneapolis.
The initiative partnered with researchers from Purdue University’s Lyles School of Civil and Construction Engineering to evaluate the practical application of upper-room germicidal UV disinfection in a real operating environment.
The goal was not simply to test a technology but to answer questions facility owners regularly face:
Can airborne infection-control upgrades be deployed economically without replacing existing HVAC systems? Can they be commissioned and validated safely with minimal disruption to residents and staff? And can they generate evidence that operators, engineers, and decision-makers consider credible?
According to Light Progress CEO Giulia Santi, the pilot reflects what facility teams observe after deploying UV-based air disinfection strategies.
That is why many senior living operators are beginning to view indoor air quality as part of their infection-prevention infrastructure, alongside cleaning protocols, vaccination programs, and clinical monitoring.
The value of prevention often appears in what doesn’t happen: fewer disruptions, fewer escalations of care, and more days where residents can live comfortably and safely within their own community.
FIELD-TESTED AND UNIVERSITY-VERIFIED
To evaluate whether better indoor air can help prevent illness and reduce care disruptions, Light Progress launched a pilot project at Cardigan Ridge, a senior living community in Minneapolis.
The initiative partnered with researchers from Purdue University’s Lyles School of Civil and Construction Engineering to evaluate the practical application of upper-room germicidal UV disinfection in a real operating environment.
The goal was not simply to test a technology but to answer questions facility owners regularly face:
Can airborne infection-control upgrades be deployed economically without replacing existing HVAC systems? Can they be commissioned and validated safely with minimal disruption to residents and staff? And can they generate evidence that operators, engineers, and decision-makers consider credible?
According to Light Progress CEO Giulia Santi, the pilot reflects what facility teams observe after deploying UV-based air disinfection strategies.
"When upper-room GUV is properly designed and installed, it improves indoor air quality and helps reduce illness transmission with very little energy impact,” Santi said, “in many buildings, it can be a more practical approach than significantly increasing outdoor air ventilation or upgrading filtration, both of which can introduce energy and comfort challenges.”
INDIPENDENT FIELD EVALUATION
To generate field-grade evidence, researchers tracked several indoor environmental and operational indicators.
These included:
These communities shared broadly similar building characteristics and mechanical systems, including:
The primary difference was the addition of airborne GUV disinfection in shared spaces at the Cardigan Ridge facility.
INFECTION CONTROL WITHOUT REPLACING HVAC SYSTEMS
For many facility owners, the largest barrier to improving infection control is capital investment.
Most portfolios can not justify replacing mechanical systems simply to improve airborne infection control.
At Cardigan Ridge, the HVAC infrastructure remained unchanged.
Instead, the project introduced UV disinfection as an additional clean-air layer aligned with the performance framework outlined in ASHRAE Standard 241: “Control of Infectious Aerosols”.
Rather than prescribing a specific technology, ASHRAE 241 defines the amount of Equivalent Clean Air (ECA) needed to reduce airborne infection risk.
This clean air can come from enhanced ventilation, filtration, or air-disinfection technologies such as germicidal UV.
That flexibility allows facilities to reach infection-risk targets without necessarily upgrading their entire HVAC system.
TARGET DEPLOYMENT IN SHARED SPACES
In September 2024, installation partner Noble Electric deployed the UV systems at the 118-unit Cardigan Ridge facility.
The strategy focused on shared indoor environments where transmission risk is typically highest.
Eleven upper-room GUV units were installed in common areas, including:
All equipment placement, commissioning, and safety validation followed NALMCO’s internationally recognized GUV certification and installation protocols.
This structured commissioning process helps engineers identify optimal installation locations and verify safe operation in occupied spaces.
By concentrating disinfection capacity where exposure risk is highest, facilities can significantly increase effective clean-air delivery while minimizing capital costs and operational disruption.
TABLE 1. shows reduced illness by 80%.
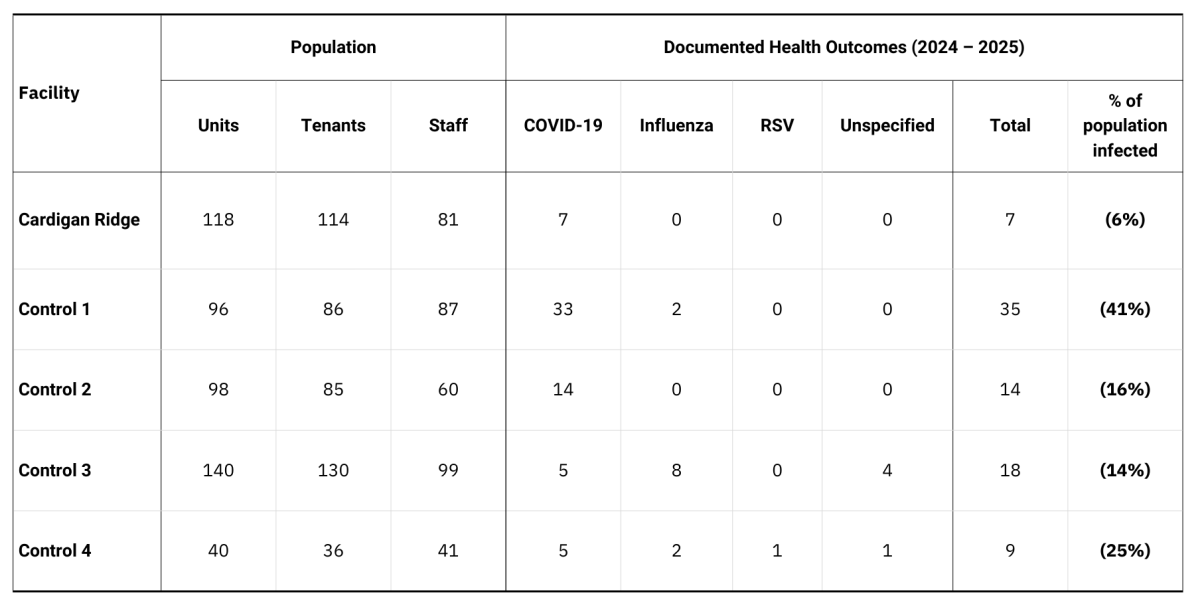
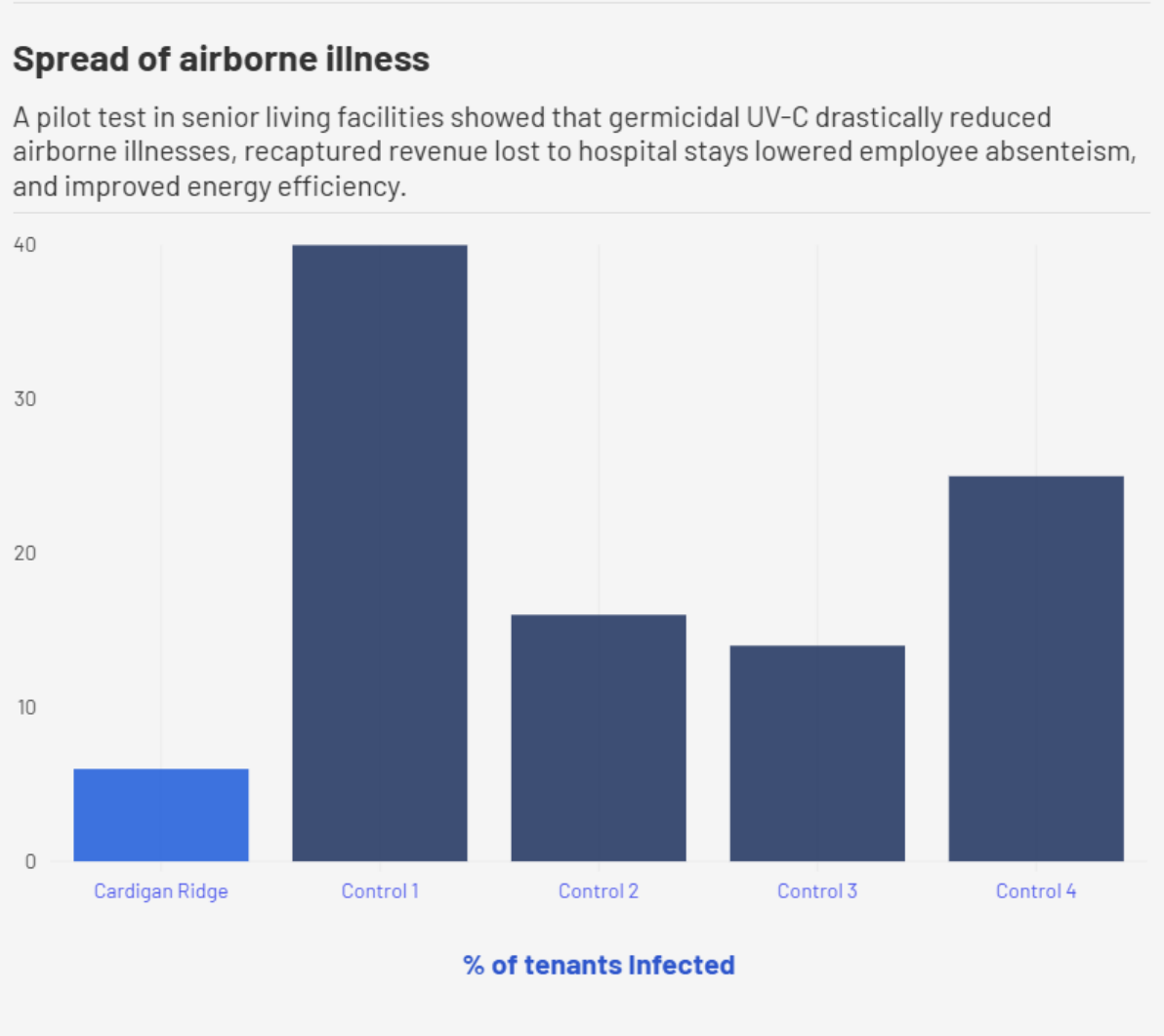
OBSERVED DIFFERENCES IN ILLNESS INCIDENCE
During the observation period, Cardigan Ridge recorded seven documented infectious disease cases among residents.
Across the four comparison communities, case counts ranged from nine to thirty-five cases.
One smaller community housing only 36 residents recorded nine cases.
While the sample size is not large enough to draw definitive clinical conclusions, the comparison suggests that targeted airborne infection-control strategies may help reduce transmission risk in shared indoor spaces.
CONCLUSION
The Cardigan Ridge pilot illustrates how airborne infection control can be integrated into existing senior living communities without replacing core HVAC infrastructure.
During the observation period, illness incidence at the facility was lower than that observed at several comparable communities.
While larger studies are needed to confirm the long-term impact of these strategies, the results support the hypothesis that properly designed UV air-disinfection systems can help reduce infection risk in indoor environments.
For operators, the practical implications are straightforward. Preventing illness has operational value.
When infections spread through a community, the consequences extend beyond resident health to include staffing disruptions, higher care intensity, and potential hospital transfers.
Reducing transmission—even modestly—can help stabilize staffing, limit disruptive care escalations, and allow more residents to remain safely supported within the community.
In that sense, targeted indoor air improvements function as infrastructure for care continuity: supporting healthier residents, steadier operations, and more predictable resource use without requiring major mechanical retrofits.
To generate field-grade evidence, researchers tracked several indoor environmental and operational indicators.
These included:
- CO₂ levels (a proxy for ventilation performance)
- thermostat and HVAC runtime data
- core IAQ parameters
- infection incidence among residents and staff
These communities shared broadly similar building characteristics and mechanical systems, including:
- resident rooms served by individual heating and cooling units
- shared spaces served by centralized ventilation systems
- approximately 25% outdoor air intake
- MERV-9 filtration
- continuously operating ventilation fans
The primary difference was the addition of airborne GUV disinfection in shared spaces at the Cardigan Ridge facility.
INFECTION CONTROL WITHOUT REPLACING HVAC SYSTEMS
For many facility owners, the largest barrier to improving infection control is capital investment.
Most portfolios can not justify replacing mechanical systems simply to improve airborne infection control.
At Cardigan Ridge, the HVAC infrastructure remained unchanged.
Instead, the project introduced UV disinfection as an additional clean-air layer aligned with the performance framework outlined in ASHRAE Standard 241: “Control of Infectious Aerosols”.
Rather than prescribing a specific technology, ASHRAE 241 defines the amount of Equivalent Clean Air (ECA) needed to reduce airborne infection risk.
This clean air can come from enhanced ventilation, filtration, or air-disinfection technologies such as germicidal UV.
That flexibility allows facilities to reach infection-risk targets without necessarily upgrading their entire HVAC system.
TARGET DEPLOYMENT IN SHARED SPACES
In September 2024, installation partner Noble Electric deployed the UV systems at the 118-unit Cardigan Ridge facility.
The strategy focused on shared indoor environments where transmission risk is typically highest.
Eleven upper-room GUV units were installed in common areas, including:
- dining spaces
- library area
- fitness rooms
- recreational and gathering spaces
All equipment placement, commissioning, and safety validation followed NALMCO’s internationally recognized GUV certification and installation protocols.
This structured commissioning process helps engineers identify optimal installation locations and verify safe operation in occupied spaces.
By concentrating disinfection capacity where exposure risk is highest, facilities can significantly increase effective clean-air delivery while minimizing capital costs and operational disruption.
TABLE 1. shows reduced illness by 80%.
OBSERVED DIFFERENCES IN ILLNESS INCIDENCE
During the observation period, Cardigan Ridge recorded seven documented infectious disease cases among residents.
Across the four comparison communities, case counts ranged from nine to thirty-five cases.
One smaller community housing only 36 residents recorded nine cases.
While the sample size is not large enough to draw definitive clinical conclusions, the comparison suggests that targeted airborne infection-control strategies may help reduce transmission risk in shared indoor spaces.
CONCLUSION
The Cardigan Ridge pilot illustrates how airborne infection control can be integrated into existing senior living communities without replacing core HVAC infrastructure.
During the observation period, illness incidence at the facility was lower than that observed at several comparable communities.
While larger studies are needed to confirm the long-term impact of these strategies, the results support the hypothesis that properly designed UV air-disinfection systems can help reduce infection risk in indoor environments.
For operators, the practical implications are straightforward. Preventing illness has operational value.
When infections spread through a community, the consequences extend beyond resident health to include staffing disruptions, higher care intensity, and potential hospital transfers.
Reducing transmission—even modestly—can help stabilize staffing, limit disruptive care escalations, and allow more residents to remain safely supported within the community.
In that sense, targeted indoor air improvements function as infrastructure for care continuity: supporting healthier residents, steadier operations, and more predictable resource use without requiring major mechanical retrofits.